Baby Has Fever With Rash on Stomach With a Cold
Rheumatic fever is a nonsuppurative, acute inflammatory complication of group A streptococcal pharyngeal infection, causing combinations of arthritis, carditis, subcutaneous nodules, erythema marginatum, and chorea. Diagnosis is based on applying the modified Jones criteria to information gleaned from history, examination, and laboratory testing. Treatment includes aspirin or other nonsteroidal anti-inflammatory drugs, corticosteroids during severe carditis, and antimicrobials to eradicate residual streptococcal infection and prevent reinfection.
Worldwide, incidence is 19/100,000 (range, 5 to 51/100,000), with lowest rates (< 10/100,000) in North America and Western Europe and highest rates (> 10/100,000) in Eastern Europe, the Middle East, Asia, Africa, Australia, and New Zealand. The attack rate (percentage of patients with untreated group A streptococcal pharyngitis who develop ARF) varies from < 1.0 to 3.0%. Higher attack rates occur with certain streptococcal M protein serotypes and a stronger host immune response (likely resulting from as-yet-uncharacterized genetic tendencies).
In patients with a prior episode of ARF, the rate of recurrence of ARF in untreated group A streptococcal pharyngitis approaches 50%, underscoring the importance of long-term antistreptococcal prophylaxis. Incidence has declined in most developed countries but remains high in less developed parts of the world, especially parts with aboriginal or native populations, such as Alaskan Native, Canadian Inuit, Native American, Australian Aboriginal, and Maori New Zealander, where incidence is as high as 50 to 250/100,000. However, the continued occurrence in the US of local outbreaks of ARF suggest that more rheumatogenic strains of streptococci are still present in the US.
The prevalence of chronic rheumatic heart disease is uncertain because criteria are not standardized and autopsy is not done routinely, but it is estimated that worldwide there are ≥ 33 million patients with rheumatic heart disease, resulting in about 300,000 deaths annually (1 General references Rheumatic fever is a nonsuppurative, acute inflammatory complication of group A streptococcal pharyngeal infection, causing combinations of arthritis, carditis, subcutaneous nodules, erythema... read more 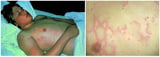 , 2 General references Rheumatic fever is a nonsuppurative, acute inflammatory complication of group A streptococcal pharyngeal infection, causing combinations of arthritis, carditis, subcutaneous nodules, erythema... read more ).
, 2 General references Rheumatic fever is a nonsuppurative, acute inflammatory complication of group A streptococcal pharyngeal infection, causing combinations of arthritis, carditis, subcutaneous nodules, erythema... read more ).
-
1. Watkins DA, Johnson CO, Colquhoun SM, et al: Global, regional, and national burden of rheumatic heart disease, 1990–2015. N Engl J Med 377:713–722, 2017. doi: 10.1056/NEJMoa1603693
Group A streptococcal (GAS) pharyngitis is the etiologic precursor of acute rheumatic fever, but host and environmental factors are important. GAS M proteins share epitopes (antigenic-determinant sites that are recognized by antibodies) with proteins found in synovium, heart muscle, and heart valve, suggesting that molecular mimicry by GAS antigens from rheumatogenic strains contributes to the arthritis, carditis, and valvular damage. Genetic host risk factors include the D8/17 B-cell antigen and certain class II histocompatibility antigens. Undernutrition, overcrowding, and lower socioeconomic status predispose to streptococcal infections and subsequent episodes of rheumatic fever.
The joints, heart, skin, and central nervous system (CNS) are most often affected. Pathology varies by site.
Joint involvement manifests as nonspecific synovial inflammation, which if biopsied sometimes shows small foci resembling Aschoff bodies (granulomatous collections of leukocytes, myocytes, and interstitial collagen). Unlike the cardiac findings, however, the abnormalities of the joints are not chronic and do not leave scarring or residual abnormalities ("ARF licks the joints but bites the heart").
Cardiac involvement manifests as carditis, typically affecting the heart from the inside out, ie, valves and endocardium, then myocardium, and finally pericardium. It is sometimes followed years to decades later by chronic rheumatic heart disease, primarily manifested by valvular stenosis, but also sometimes by regurgitation, arrhythmias, and ventricular dysfunction.
In acute rheumatic fever, Aschoff bodies often develop in the myocardium and other parts of the heart. Fibrinous nonspecific pericarditis, sometimes with effusion, occurs only in patients with endocardial inflammation and usually subsides without permanent damage. Characteristic and potentially dangerous valve changes may occur. Acute interstitial valvulitis may cause valvular edema.
In chronic rheumatic heart disease, valve thickening, fusion, and retraction or other destruction of leaflets and cusps may occur, leading to stenosis or insufficiency. Similarly, chordae tendineae can shorten, thicken, or fuse, worsening regurgitation of damaged valves or causing regurgitation of an otherwise unaffected valve. Dilation of valve rings may also cause regurgitation.
Rheumatic valvular disease most commonly involves the mitral and aortic valves. The tricuspid and pulmonic valves are seldom if ever affected in isolation.
In acute rheumatic fever, the most common cardiac manifestations are
-
Mitral regurgitation
-
Pericarditis
-
Sometimes aortic regurgitation
In chronic rheumatic heart disease, the most common cardiac manifestations are
-
Mitral stenosis
-
Aortic regurgitation (often with some degree of stenosis)
-
Perhaps tricuspid regurgitation (often along with mitral stenosis)
Subcutaneous nodules appear indistinguishable from those of juvenile idiopathic arthritis Juvenile Idiopathic Arthritis (JIA) Juvenile idiopathic arthritis is a group of rheumatic diseases that begins by age 16. Arthritis, fever, rash, adenopathy, splenomegaly, and iridocyclitis are typical of some forms. Diagnosis... read more  (JIA), but biopsy shows features resembling Aschoff bodies. Erythema marginatum differs histologically from other skin lesions with similar macroscopic appearance, eg, the rash of systemic JIA, immunoglobulin A–associated vasculitis (formerly called Henoch-Schönlein purpura), erythema chronicum migrans, and erythema multiforme. Perivascular neutrophilic and mononuclear infiltrates of the dermis occur.
(JIA), but biopsy shows features resembling Aschoff bodies. Erythema marginatum differs histologically from other skin lesions with similar macroscopic appearance, eg, the rash of systemic JIA, immunoglobulin A–associated vasculitis (formerly called Henoch-Schönlein purpura), erythema chronicum migrans, and erythema multiforme. Perivascular neutrophilic and mononuclear infiltrates of the dermis occur.
Sydenham chorea, the form of chorea that occurs with ARF, manifests in the CNS as hyperperfusion and increased metabolism in the basal ganglia. Increased levels of antineuronal antibodies have also been shown.
Symptoms and Signs of Rheumatic Fever
Joints
Migratory polyarthritis is the most common manifestation of acute rheumatic fever, occurring in about 35 to 66% of children; it is often accompanied by fever. "Migratory" means the arthritis appears in one or a few joints, resolves but then appears in others, thus seeming to move from one joint to another. Occasionally monarthritis occurs in high-risk indigenous populations (eg, in Australia, India, Fiji) but very rarely in the US. Joints become extremely painful and tender; these symptoms are often out of proportion to the modest warmth and swelling present on examination (this is in contrast to the arthritis of Lyme disease Lyme Disease Lyme disease is a tick-transmitted infection caused by the spirochete Borrelia species. Early symptoms include an erythema migrans rash, which may be followed weeks to months later by neurologic... read more  , in which the examination findings tend to be more severe than the symptoms).
, in which the examination findings tend to be more severe than the symptoms).
Ankles, knees, elbows, and wrists are usually involved. Shoulders, hips, and small joints of the hands and feet also may be involved, but almost never alone. If vertebral joints are affected, another disorder should be suspected.
Arthralgia-like symptoms may be due to nonspecific myalgia or tenodynia in the periarticular zone; tenosynovitis may develop at the site of muscle insertions. Joint pain and fever usually subside within 2 weeks and seldom last > 1 month.
Heart
Carditis can occur alone or in combination with pericardial rub, murmurs, cardiac enlargement, or heart failure. In the first episode of acute rheumatic fever, carditis occurs in about 50 to 70%. Patients may have high fever, chest pain, or both; tachycardia is common, especially during sleep. In about 50% of cases, cardiac damage (ie, persistent valve dysfunction) occurs much later.
Although the carditis of ARF is considered to be a pancarditis (involving the endocardium, myocardium, and pericardium), valvulitis is the most consistent feature of ARF, and if it is not present, the diagnosis should be reconsidered. The diagnosis of valvulitis has classically been made by auscultation of murmurs, but subclinical cases (ie, valvular dysfunction not manifested by murmurs but recognized on echocardiography and Doppler studies) may occur in up to 18% of cases of ARF.
Heart murmurs are common and, although usually evident early, may not be heard at initial examination; in such cases, repeated clinical examinations as well as echocardiography are recommended to determine the presence of carditis. Mitral regurgitation is characterized by an apical pansystolic blowing murmur radiating to the axilla. The soft diastolic blow at the left sternal border of aortic regurgitation, and the presystolic murmur of mitral stenosis, may be difficult to detect. Murmurs often persist indefinitely. If no worsening occurs during the next 2 to 3 weeks, new manifestations of carditis seldom follow. ARF typically does not cause chronic, smoldering carditis. Scars left by acute valvular damage may contract and change, and secondary hemodynamic difficulties may develop in the myocardium without persistence of acute inflammation.
Pericarditis may be manifested by chest pain and a pericardial rub.
Heart failure caused by the combination of carditis and valvular dysfunction may cause dyspnea without rales, nausea and vomiting, a right upper quadrant or epigastric ache, and a hacking, nonproductive cough. Marked lethargy and fatigue may be early manifestations of heart failure.
Skin
Cutaneous and subcutaneous features are uncommon and almost never occur alone, usually developing in a patient who already has carditis, arthritis, or chorea.
Subcutaneous nodules, which occur most frequently on the extensor surfaces of large joints (eg, knees, elbows, wrists), usually coexist with arthritis and carditis. Fewer than 10% of children with acute rheumatic fever have nodules. Ordinarily, the nodules are painless and transitory and respond to treatment of joint or heart inflammation.
Erythema marginatum is a serpiginous, flat or slightly raised, nonscarring, and painless rash. Fewer than 6% of children have this rash. The rash usually appears on the trunk and proximal extremities but not the face. It sometimes lasts < 1 day. Its appearance is often delayed after the inciting streptococcal infection; it may appear with or after the other manifestations of rheumatic inflammation.
CNS
Characteristic findings include fluctuating grip strength (milkmaid's grip), tongue fasciculations or tongue darting (the tongue cannot protrude without darting in and out), facial grimacing, and explosive speech with or without tongue clucking. Associated motor symptoms include loss of fine motor control, and weakness and hypotonia (that can be severe enough to be mistaken for paralysis).
Other
Fever (≥ 38.5° C) and other systemic manifestations such as anorexia and malaise can be prominent but are not specific. ARF can occasionally manifest as fever of unknown origin until a more identifiable sign develops. Abdominal pain and anorexia can occur because of the hepatic involvement in heart failure or because of concomitant mesenteric adenitis, and rarely the situation may resemble acute appendicitis.
Recurrence
Recurrent episodes of ARF often mimic the initial episode; carditis tends to recur in patients who have had moderate to severe carditis in the past, and chorea without carditis recurs in patients who had chorea without carditis initially.
Symptoms and signs reference
-
1. Gewitz MH, Baltimore RS, Tani LY, et al: Revision of Jones criteria for the diagnosis of acute rheumatic fever in the era of Doppler echocardiography: A scientific statement from the American Heart Association. Circulation 131:1806–1818, 2015. doi: 10.1161/CIR.0000000000000205
-
Modified Jones criteria (for initial diagnosis)
-
Testing for GAS (culture, rapid strep test, or antistreptolysin O and anti-DNase B titers)
-
ECG
-
Echocardiography with Doppler
-
Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level
Diagnosis of a first episode of acute rheumatic fever (ARF) is based on the modified Jones criteria (1 Diagnosis reference Rheumatic fever is a nonsuppurative, acute inflammatory complication of group A streptococcal pharyngeal infection, causing combinations of arthritis, carditis, subcutaneous nodules, erythema... read more ; see Table: Modified Jones Criteria for a First Episode of Acute Rheumatic Fever (ARF)* Modified Jones Criteria for a First Episode of Acute Rheumatic Fever (ARF)* Rheumatic fever is a nonsuppurative, acute inflammatory complication of group A streptococcal pharyngeal infection, causing combinations of arthritis, carditis, subcutaneous nodules, erythema... read more ); 2 major criteria or 1 major and 2 minor criteria are required, each along with evidence of preceding group A streptococcal (GAS) infection. Sydenham chorea alone (ie, without minor criteria) fulfills diagnostic criteria if other causes of movement disorder are ruled out.
The modified Jones criteria were designed for the evaluation of acute rheumatic fever rather than for a possible recurrence. However, if patients have a reliable past history of acute rheumatic fever or rheumatic heart disease and also have documented group A streptococcal infection, the criteria may be used to establish the presence of a recurrence.
A preceding streptococcal infection is suggested by a recent history of pharyngitis and is confirmed by one or more of the following:
-
Positive throat culture
-
Increased or preferably rising antistreptolysin O titer
-
Positive rapid GAS antigen test in a child with clinical manifestations suggestive of streptococcal pharyngitis
Joint aspiration may be needed to exclude other causes of arthritis (eg, infection). The joint fluid is usually cloudy and yellow, with an elevated white blood cell (WBC) count composed primarily of neutrophils; culture is negative. Complement levels are usually normal or slightly decreased, compared with decreased levels in other inflammatory arthritides.
ECG is done during the initial evaluation. Serum cardiac marker levels are obtained; normal cardiac troponin I levels exclude prominent myocardial damage. ECG abnormalities such as PR prolongation do not correlate with other evidence of carditis. Only 35% of children with ARF have a prolonged PR interval; higher-degree heart block may occur but is uncommon. Other ECG abnormalities may be due to pericarditis, enlargement of ventricles or atria, or arrhythmias.
Echocardiography can detect evidence of carditis even in patients without apparent murmurs and is recommended for all patients with confirmed or suspected ARF. Echocardiography is also used to detect subclinical carditis in patients with apparently isolated Sydenham chorea and to monitor the status of patients with recurrences of carditis or chronic rheumatic heart disease. However, not all echocardiographic abnormalities represent rheumatic carditis; isolated trivial valvar regurgitation or trivial pericardial effusion may be a nonspecific finding. To maintain specificity, echocardiographic and Doppler results should meet the following criteria (1 Diagnosis reference Rheumatic fever is a nonsuppurative, acute inflammatory complication of group A streptococcal pharyngeal infection, causing combinations of arthritis, carditis, subcutaneous nodules, erythema... read more ) for acute rheumatic carditis:
Doppler flow criteria:
-
Pathologic mitral regurgitation: Must be seen in at least 2 views, and have a jet length ≥ 2 cm in at least 1 view, a peak velocity of > 3 m/second, and a pansystolic jet in at least 1 envelope
-
Pathologic aortic regurgitation: Must be seen in at least 2 views, and have a jet length ≥ 1 cm in at least 1 view, a peak velocity of > 3 m/second, and a pandiastolic jet in at least 1 envelope
Echocardiographic morphologic criteria:
-
Pathologic mitral valve morphologic changes include annular dilation, chordal elongation or rupture with flail leaflet, anterior (or less commonly posterior) leaflet tip prolapse, or beading/nodularity of leaflet tips.
-
Pathologic aortic valve morphologic changes include irregular or focal leaflet thickening, coaptation defect, restricted leaflet motion, or leaflet prolapse.
Chest x-rays are not routinely done but can detect cardiomegaly, a common manifestation of carditis in ARF.
Biopsy of a subcutaneous nodule can aid in early diagnosis, especially when other major clinical manifestations are absent.
ESR and serum CRP are sensitive but not specific. The ESR is typically > 60 mm/hour. CRP is typically > 30 mg/L (> 285.7 nmol/L) and often > 70 mg/L (> 666.7 nmol/L); because it rises and falls faster than ESR, a normal CRP may confirm that inflammation is resolving in a patient with prolonged ESR elevation after acute symptoms have subsided. In the absence of carditis, ESR usually returns to normal within 3 months. Evidence of acute inflammation, including ESR, usually subsides within 5 months in uncomplicated carditis. The WBC count reaches 12,000 to 20,000/mcL (12 to 20 × 109/L) and may go higher with corticosteroid therapy.
The differential diagnosis includes JIA Juvenile Idiopathic Arthritis (JIA) Juvenile idiopathic arthritis is a group of rheumatic diseases that begins by age 16. Arthritis, fever, rash, adenopathy, splenomegaly, and iridocyclitis are typical of some forms. Diagnosis... read more (especially systemic JIA and, less so, polyarticular JIA), Lyme disease Diagnosis Lyme disease is a tick-transmitted infection caused by the spirochete Borrelia species. Early symptoms include an erythema migrans rash, which may be followed weeks to months later by neurologic... read more , reactive arthritis Diagnosis Reactive arthritis is an acute spondyloarthropathy that often seems precipitated by an infection, usually genitourinary or gastrointestinal. Common manifestations include asymmetric arthritis... read more  , arthropathy of sickle cell disease, leukemia Overview of Leukemia Leukemia is a malignant condition involving the excess production of immature or abnormal leukocytes, which eventually suppresses the production of normal blood cells and results in symptoms... read more or other cancer, systemic lupus erythematosus Diagnosis Systemic lupus erythematosus is a chronic, multisystem, inflammatory disorder of autoimmune etiology, occurring predominantly in young women. Common manifestations may include arthralgias and... read more
, arthropathy of sickle cell disease, leukemia Overview of Leukemia Leukemia is a malignant condition involving the excess production of immature or abnormal leukocytes, which eventually suppresses the production of normal blood cells and results in symptoms... read more or other cancer, systemic lupus erythematosus Diagnosis Systemic lupus erythematosus is a chronic, multisystem, inflammatory disorder of autoimmune etiology, occurring predominantly in young women. Common manifestations may include arthralgias and... read more  , embolic bacterial endocarditis Diagnosis Infective endocarditis is infection of the endocardium, usually with bacteria (commonly, streptococci or staphylococci) or fungi. It may cause fever, heart murmurs, petechiae, anemia, embolic... read more
, embolic bacterial endocarditis Diagnosis Infective endocarditis is infection of the endocardium, usually with bacteria (commonly, streptococci or staphylococci) or fungi. It may cause fever, heart murmurs, petechiae, anemia, embolic... read more  , serum sickness Drug Hypersensitivity Drug hypersensitivity is an immune-mediated reaction to a drug. Symptoms range from mild to severe and include rash, anaphylaxis, and serum sickness. Diagnosis is clinical; skin testing is occasionally... read more , Kawasaki disease Diagnosis Kawasaki disease is a vasculitis, sometimes involving the coronary arteries, that tends to occur in infants and children between the ages of 1 year and 8 years. It is characterized by prolonged... read more
, serum sickness Drug Hypersensitivity Drug hypersensitivity is an immune-mediated reaction to a drug. Symptoms range from mild to severe and include rash, anaphylaxis, and serum sickness. Diagnosis is clinical; skin testing is occasionally... read more , Kawasaki disease Diagnosis Kawasaki disease is a vasculitis, sometimes involving the coronary arteries, that tends to occur in infants and children between the ages of 1 year and 8 years. It is characterized by prolonged... read more  , drug reactions Diagnosis Drugs can cause multiple skin eruptions and reactions. The most serious of these are discussed elsewhere in THE MANUAL and include Stevens-Johnson syndrome and toxic epidermal necrolysis, hypersensitivity... read more
, drug reactions Diagnosis Drugs can cause multiple skin eruptions and reactions. The most serious of these are discussed elsewhere in THE MANUAL and include Stevens-Johnson syndrome and toxic epidermal necrolysis, hypersensitivity... read more  , and gonococcal arthritis Gonococcal arthritis Acute infectious arthritis is a joint infection that evolves over hours or days. The infection resides in synovial or periarticular tissues and is usually bacterial—in younger adults, frequently... read more
, and gonococcal arthritis Gonococcal arthritis Acute infectious arthritis is a joint infection that evolves over hours or days. The infection resides in synovial or periarticular tissues and is usually bacterial—in younger adults, frequently... read more  . These are frequently distinguished by history or specific laboratory tests. The absence of an antecedent GAS infection, the diurnal variation of the fever, evanescent rash, and prolonged symptomatic joint inflammation usually distinguish systemic JIA from ARF.
. These are frequently distinguished by history or specific laboratory tests. The absence of an antecedent GAS infection, the diurnal variation of the fever, evanescent rash, and prolonged symptomatic joint inflammation usually distinguish systemic JIA from ARF.
![]()
-
1. Gewitz MH, Baltimore RS, Tani LY, et al: Revision of Jones criteria for the diagnosis of acute rheumatic fever in the era of Doppler echocardiography: A scientific statement from the American Heart Association. Circulation 131:1806–1818, 2015. doi: 10.1161/CIR.0000000000000205
Prognosis following an initial episode of acute rheumatic fever depends mostly on how severely the heart is affected, and whether there is a recurrent episode of acute rheumatic fever. Murmurs eventually disappear in about half of patients whose acute episodes were manifested by mild carditis without major cardiac enlargement or decompensation. However, many others develop chronic valvular disease, including some who recovered from the acute episode without evidence of valvular disease.
Episodes of Sydenham chorea usually last several months and resolve completely in most patients, but about one third of patients have recurrences.
Joint inflammation may take 1 month to subside if not treated but does not lead to residual damage.
In patients with chronic valvular disease, symptoms develop and progress slowly, typically over several decades. However, once significant symptoms develop, intervention is usually necessary. In developing countries, chronic rheumatic heart disease is the cause of 25 to 45% of all cardiovascular disease.
-
Antibiotics
-
Aspirin
-
Sometimes corticosteroids
The primary goals of rheumatic fever treatment are eradication of group A streptococcal infection, relief of acute symptoms, suppression of inflammation, and prophylaxis against future infection to prevent recurrent heart disease.
For general management, patients should limit their activities if they have symptoms of arthritis, chorea, or heart failure. In the absence of carditis, no physical restrictions are needed after the initial episode subsides. In asymptomatic patients with carditis, strict bed rest has no proven value, despite its traditional usage.
Although poststreptococcal inflammation is well developed by the time ARF is detected, a 10-day course of oral penicillin or amoxicillin, or a single injection of benzathine penicillin, is used to eradicate any lingering organisms and prevent reinfection. For specific regimens, see treatment of streptococcal pharyngitis Pharyngitis Streptococci are gram-positive aerobic organisms that cause many disorders, including pharyngitis, pneumonia, wound and skin infections, sepsis, and endocarditis. Symptoms vary with the organ... read more  . Antibiotic prophylaxis Antibiotic prophylaxis Rheumatic fever is a nonsuppurative, acute inflammatory complication of group A streptococcal pharyngeal infection, causing combinations of arthritis, carditis, subcutaneous nodules, erythema... read more is continued as described below.
. Antibiotic prophylaxis Antibiotic prophylaxis Rheumatic fever is a nonsuppurative, acute inflammatory complication of group A streptococcal pharyngeal infection, causing combinations of arthritis, carditis, subcutaneous nodules, erythema... read more is continued as described below.
Aspirin controls fever and pain and should be given to all patients with arthritis and/or mild carditis. Although aspirin has been used for many decades, there are surprisingly few data from controlled trials to define the optimal dosing schedule. Most experts would give children and adolescents 15 to 25 mg/kg orally 4 times a day (to a maximum daily dose of 4 to 6 g) for 2 to 4 weeks and then taper the dose over another 4 weeks. Symptomatic ARF responds dramatically to aspirin. If no improvement is seen after 24 to 48 hours of high-dose aspirin therapy, the diagnosis of ARF should be reconsidered. Salicylate toxicity Aspirin and Other Salicylate Poisoning Salicylate poisoning can cause vomiting, tinnitus, confusion, hyperthermia, respiratory alkalosis, metabolic acidosis, and multiple organ failure. Diagnosis is clinical, supplemented by measurement... read more is the limiting factor to aspirin therapy and is manifested by tinnitus, headache, or hyperpnea; it may not appear until after 1 week of therapy. Salicylate levels are measured only to manage toxicity. Enteric-coated, buffered, or complex salicylate molecules provide no advantage.
For patients with minimal to mild carditis, there are no controlled data to suggest that adding prednisone to aspirin therapy speeds resolution of illness or prevents rheumatic heart disease.
Other nonsteroidal anti-inflammatory drugs (NSAIDs) have been reported in small trials to be effective; naproxen (7.5 to 10 mg/kg orally 2 times a day) is the most studied. However, other NSAIDs have few advantages over aspirin, especially in the first week of therapy when salicylism is uncommon. Acetaminophen is not effective for symptoms of acute rheumatic fever.
Prednisone 1 mg/kg orally 2 times a day (up to 60 mg/day) is recommended instead of aspirin for patients with moderate to severe carditis (as judged by a combination of clinical findings, presence of cardiac enlargement, and possibly by severely abnormal echocardiography results). If inflammation is not suppressed after 2 days or for severe heart failure, an IV corticosteroid pulse of methylprednisolone succinate (30 mg/kg IV once a day, maximum 1 g/day, for 3 successive days) may be given. Oral corticosteroids typically are given for 2 to 4 weeks and then tapered over another 2 to 3 weeks. Aspirin should be started during the corticosteroid taper and continued for 2 to 4 weeks after the corticosteroid has been stopped. Aspirin dose is the same as above. Inflammatory markers such as Erythrocyte sedimentation rate and C-reactive protein may be used to monitor disease activity and response to treatment.
Recurrences of mild cardiac inflammation (indicated by fever or chest pain) may subside spontaneously; aspirin or corticosteroids should be resumed if recurrent symptoms last longer than a few days or if heart failure is uncontrolled by standard management (eg, diuretics, angiotensin-converting enzyme inhibitors, beta-blockers, inotropic agents).
The optimal duration of antistreptococcal prophylaxis is uncertain. Children without carditis should receive prophylaxis for 5 years or until age 21 (whichever is longer). The American Academy of Pediatrics recommends that patients with carditis without evidence of residual heart damage receive prophylaxis for 10 years or until age 21 (whichever is longer). Children with carditis and evidence of residual heart damage should receive prophylaxis for > 10 years; many experts recommend that such patients continue prophylaxis indefinitely or, alternatively, until age 40. Prophylaxis should be life long in all patients with severe valvular disease who have close contact with young children because young children have a high rate of GAS carriage.
Recommended Prophylaxis Against Recurrent Group A Streptococcal Infection
| Regimen | Drug | Dosage |
|---|---|---|
| Standard | Penicillin G benzathine | 1.2 million units IM every 3–4 weeks* ≤ 27 kg: 600,000 units IM every 3–4 weeks* |
| Alternatives (eg, for patients unwilling to receive injections) | Penicillin V or Sulfadiazine or Sulfisoxazole | 250 mg orally 2 times a day ≤ 27 kg: 500 mg orally once a day > 27 kg: 1 g orally once a day |
| For patients allergic to penicillin and sulfa drugs | Erythromycin or Azithromycin | 250 mg orally 2 times a day 250 mg orally once a day |
| * In parts of the world with high acute rheumatic fever endemicity, IM prophylaxis every 3 weeks is superior to every 4 weeks. | ||
-
Rheumatic fever is a nonsuppurative, acute, inflammatory complication of group A streptococcal (GAS) pharyngeal infection occurring most often initially between ages 5 years and 15 years.
-
Symptoms and signs may include migratory polyarthritis, carditis, subcutaneous nodules, erythema marginatum, and chorea.
-
Chronic rheumatic heart disease, particularly involving the mitral and/or aortic valves, may progress over decades and is a major cause of heart disease in the developing world.
-
Give antibiotics to eliminate GAS infection, aspirin to control fever and pain caused by arthritis and mild carditis, and corticosteroids for patients with moderate to severe carditis.
-
Give prophylactic antistreptococcal antibiotics after the initial episode of ARF to prevent recurrences.
Poststreptococcal reactive arthritis may or may not represent an attenuated variant of acute rheumatic fever (ARF). Patients do not have symptoms or signs of the carditis common in ARF.
Compared with the arthritis of ARF, poststreptococcal reactive arthritis typically involves only 1 or 2 joints, is less migratory but more protracted, and does not respond as well or as quickly to aspirin. Other, nonrheumatic disorders causing similar symptoms (eg, Lyme arthritis Diagnosis Lyme disease is a tick-transmitted infection caused by the spirochete Borrelia species. Early symptoms include an erythema migrans rash, which may be followed weeks to months later by neurologic... read more , juvenile idiopathic arthritis Juvenile Idiopathic Arthritis (JIA) Juvenile idiopathic arthritis is a group of rheumatic diseases that begins by age 16. Arthritis, fever, rash, adenopathy, splenomegaly, and iridocyclitis are typical of some forms. Diagnosis... read more ) should be excluded.
It can be treated with other nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen and naproxen.
Although clinical practice for secondary prevention of cardiac involvement varies greatly, it is reasonable to give antistreptococcal prophylaxis for several months to 1 year and then to reevaluate the patient. If cardiac lesions are detected by echocardiography, long-term prophylaxis is indicated.
Baby Has Fever With Rash on Stomach With a Cold
Source: https://www.msdmanuals.com/professional/pediatrics/miscellaneous-bacterial-infections-in-infants-and-children/rheumatic-fever
0 Response to "Baby Has Fever With Rash on Stomach With a Cold"
Post a Comment